
Cardizem
By I. Folleck. Mississippi University for Women. 2018.
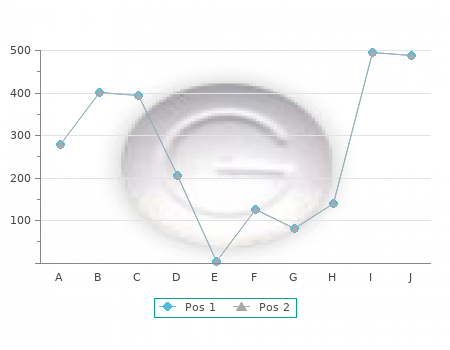
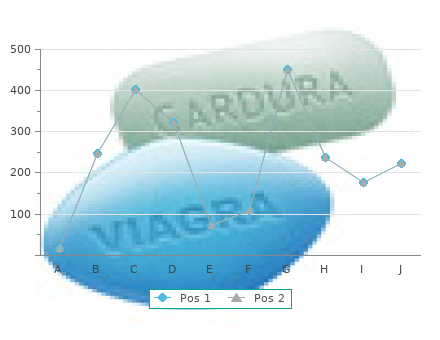
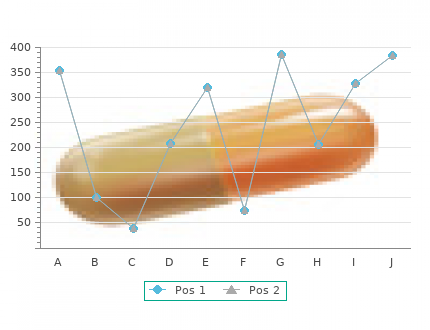
Our model of the dorsal visual stream included the lateral FIGURE 29 cardizem 180 mg on-line blood pressure medication hydro. This graph shows the correlation between the temporal index of geniculate nucleus buy generic cardizem 180mg online hypertension range, V1, V5, and the PP. Although connec- changes in effective connectivity and learning. The temporal tions between regions are generally reciprocal, for simplicity index is defined as the time of a maximum increase in effective we modeled only unidirectional paths. For example, a temporal index of 3 indicates To assess effective connectivity in a condition-specific that the maximum increase in effective connectivity occurred be- fashion, we used time series that comprised observations tween the third and fourth blocks. The numbers denote the sub- during the condition in question. Path coefficients for both ject from which this temporal index of effective connectivity was obtained. Each subject was scanned during three independent conditions (attention and no attention) were estimated by learning sessions; therefore, each number appears three times. To test for the im- A negative slope means that the maximum increase in effective pact of changes in effective connectivity between attention connectivity occurs earlier in fast learning. The predictive value of changes in effective connec- and no attention, we defined a free model (allowing different tivity for human learning. Science 1999;283:1538–1541, with per- path coefficients between V1 and V5 for attention and no mission. The connectivity be- tween V1 and V5 increases significantly during attention. The specific hypothesis we addressed was that parietal cortex could modulate the inputs from V1 to V5. The experiment was performed on a 2-T MRI system equipped with a head volume coil. The subject was scanned during four dif- ferent conditions: fixation, attention, no attention, and sta- tionary. Each condition lasted 32 seconds to give 10 volumes per condition. During all conditions, the subjects looked at a fixation point in the middle of a screen. In this section, we are interested only in the two conditions with visual motion (attention and no attention), in which 250 small white dots moved radially from the fixation point, in random directions, toward the border of the screen at a constant speed of 4. The difference between attention and no attention lay in the explicit command given to the subject shortly before the condition: just look indicated no attention, and FIGURE 29. Structural equation model of the dorsal visual pathway, comparing attention and no attention. Connectivity be- detect changes indicated the attention condition. Both visual tween right primary visual cortex (V1) and motion-sensitive area motion conditions were interleaved with fixation. No re- (V5) is increased during attention relative to no attention. Effective connectivity¨ Regions of interest were defined by categoric compari- in functional brain imaging. Neural Networks 2000;13:871–882, sons with use of an output statistical image (SPM Z ) com- with permission. This can be tested by splitting the observations into two sets, one containing observations in which the PP activity is high and another one in which the PP activity is low. It is now possible to perform separate regressions of V5 on V1 by using both sets. If the hypothesis of positive modula- tion is true, the slope of the regression of V5 on V1 should be steeper under high values of PP. Variable Parameter Regression As demonstrated in the previous sections, the basic linear model can be seen as a linear regression. Structural equation model of the dorsal visual coefficient is then interpreted as a measure of the connectiv- pathway incorporating the interaction effect of right posterior parietal cortex on the connection from right primary visual cortex ity between areas. This interpretation of course implies that (V1) to motion-sensitive area (V5). Neural Net- effective strength equal to the regression coefficient.
Summary of strength of evidence and effect estimate for KQ 5—pharmacological rhythm-control therapies Treatment Restoration of Maintenance of Recurrence of All-Cause and AF and CV Heart Failure Quality of Life Stroke (and Bleeding Comparison Sinus Rhythm Sinus Rhythm AF CV Mortality Hospitaliza- Symptoms/ Mixed Embolic Events tions Control of AF Events discount 180mg cardizem fast delivery heart attack jack ps baby, Symptoms Including Stroke) Pharmaco- SOE = SOE = SOE = All-cause: SOE SOE = SOE = SOE= Stroke: SOE = SOE = logical therapy Insufficient (no Insufficient (1 Insufficient (4 = Insufficient (1 Insufficient (no Insufficient (no Insufficient (1 Insufficient (1 Insufficient (no in which studies) study purchase cardizem 180 mg online blood pressure chart print out, 168 studies, 414 study, 168 studies) studies) study, 144 study, 168 studies) electrical patients) patients) patients) patients) patients) cardioversion is a key Cardiac: SOE = Mixed: SOE = component of Insufficient (no Insufficient (no the treatment studies) studies) Comparison of SOE = SOE = Low (9 SOE = Low (10 All-cause: SOE CV: SOE = Heart failure: SOE = Low (2 Stroke: SOE = SOE = pharmaco- Insufficient (no studies, 2,095 studies, 3,223 = Insufficient (5 Insufficient (no SOE = studies, 1,068 Insufficient (2 Insufficient (no logical agents studies) patients) patients) studies, 2,076 studies) Insufficient (no patients) studies, 1,068 studies) Amiodarone Amiodarone patients) studies) No significant patients) appears to be appears to be AF: SOE = Low difference was better than better than Cardiac: SOE = (1 study, 403 AF symptoms: found in either Mixed: SOE = sotalol but no dronedarone or Low (4 studies, patients) SOE = Low (1 study. Insufficient (no different from sotalol but no 1,664 patients) Rate and mean study, 403 studies) propafenone. Note: AF = atrial fibrillation; CV = cardiovascular; KQ = Key Question; SOE = strength of evidence. Rate- Versus Rhythm-Control Therapies Key points from the Results chapter of the full report are as follows. This finding is based on evidence from four RCTs (two good, two fair quality) involving 1,700 patients (low strength of evidence). A total of 14 RCTs were included in our analysis, 12 that explored a rhythm-control strategy using pharmacological therapy versus a rate-control strategy and 2 that compared a rhythm- control strategy with PVI versus a rate-control strategy that involved AVN ablation and implantation of a pacemaker in one case and rate-controlling medications in the other. Nine studies were of good quality, three were of fair quality, and two were of poor quality. Ten studies were conducted in continental Europe; 1 was conducted in the United States and Canada only; 1 was conducted in Asia only; 1 was conducted in the United States, Canada, South America, and Israel; and 1 study did not report the location. The number of patients included ranged from 41 to 4,060, for a total of 7,556 patients across the 14 studies. The mean age of study participants ranged from 39 years to 72 years. Five studies included only patients with persistent AF, one study included only patients with paroxysmal AF, two studies included both patients with paroxysmal and those with persistent AF, and six studies did not explicitly report type of AF. Four studies included only patients with heart failure. ES-27 Table H summarizes the strength of evidence for the rate- and rhythm-control therapies and evaluated outcomes. Details about the specific components of these ratings (risk of bias, consistency, directness, and precision) are available in the full report. Summary of strength of evidence and effect estimate for KQ 6—rate- versus rhythm- control strategies Outcome Strength of Evidence and Effect Estimate Maintenance of sinus Using AADs for rhythm control: rhythm SOE = High (7 studies, 1,473 patients) OR 0. Since 6 of the 8 studies had ORs that crossed 1 (including 95% of the patients) and given significant heterogeneity, we assessed these studies as demonstrating no difference between rate- and rhythm- control strategies. CV mortality Using AADs for rhythm control: SOE = Moderate (5 studies, 2,405 patients) OR 0. ES-28 Discussion Key Findings In this Comparative Effectiveness Review, we reviewed 148 studies represented by 182 publications and involving 25,524 patients that directly compared rate- and rhythm-control strategies in patients with AF. Although the ultimate goal with any therapy for AF is to improve long-term survival and quality of life, most studies to date have assessed rate control, conversion of AF to sinus rhythm, or maintenance of sinus rhythm. Very few studies focused on final outcomes such as survival, or on the relationship between intermediate outcomes such as ventricular rate or duration of sinus rhythm and final outcomes. For KQ 1, despite strongly held convictions among clinicians about the superiority of individual beta blockers and calcium channel blockers, we found insufficient data to support any of these claims. Based on a limited number of comparative studies, our analysis suggests that either a calcium channel blocker (verapamil or diltiazem) or amiodarone is beneficial compared with digoxin for rate control. Given the widespread use of beta blockers and calcium channel blockers and the population-level impact of even small differences in safety and effectiveness, research comparing individual drugs in different patient populations is needed. For KQ 2, by emphasizing the limitations in the available data and the paucity of data on lenient versus strict rate control, our findings highlight the need for more research in this area. For KQ 3, our findings underscore the need for additional studies to compare rate-control drugs with rate-control procedures in relation to exercise capacity, mortality, cardiovascular events, and quality of life. For KQ 4, although health care providers often debate the superiority of one positioning of cardioversion electrodes over another, we found that both positions gave comparable results, albeit with low strength of evidence. While data suggest that drug pretreatment enhances electrical cardioversion in terms of restoration and maintenance of sinus rhythm, our review does not support the current assumption that one AAD is clearly superior to others in such pretreatment. This finding challenges the assumption that one antiarrhythmic medication is clearly superior to others and underscores the need for more studies comparing the effectiveness and safety of different AADs in enhancing restoration of sinus rhythm.
J Am Acad Child in health first-degree relatives of patients with panic disorder discount 60 mg cardizem with visa arteria y vena esplenica. Hypersensitivity to carbon dioxide as a disease-spe- of depressed parents: ten years later cheap 180mg cardizem otc pulse pressure 50 mmhg. Behavioral inhibition social phobia: effects of comorbidity on familial transmission. Vulnerability between panic disorder and unipolar depression. J Psychiatr Res factors among children at risk for anxiety disorders. Biological studies on off- familial aggregation of alcoholism and anxiety disorders. Social phobia and the persis- major perspectives and findings. Clin Psychol Rev 2000;20: tence of conduct problems. In: Jones WH, childhood—a genetic study of comorbidity. Shyness: perspectives on research and chiatry 1997;38:651–656. Psychopathology of ety and depression symptoms: a genetic analysis of the effects social phobia and comparison to avoidant personality disorder. Stable behav- agoraphobia with and without comorbid major depression. Psy- ioral inhibition and its association with anxiety disorder. Does shy-inhibited tempera- among children of adults with panic disorder. In: Dunner DL, ment in childhood lead to anxiety problems in adolescence? Anxiety disorders in children anxiety frequency and the prediction of fearfulness. New York: Guil- depression and anxiety: mechanisms of psychiatric disorder. Psychological approaches to panic disorder: a re- 65. The role of anxiety sensitivity Psychiatry 1997;36:918–924. Psychophysiological assessment of anxious emo- neous panic attacks during acute stress. Anxiety sensitivity in control in children of agoraphobic parents. J Child Psychol Psy- children at risk for psychopathology. J Consulting and Clinical chiatry Allied Disc 1996;37:445–452. Chapter 61: Genetic and Other Vulnerability Factors for Anxiety and Stress Disorders 881 90. Heritability of anxiety sensitiv- development of posttraumatic stress disorder. Are different parts of the extended amygdala involved attacks in adolescents. J Am Acad Child Adolesc Psychiatry 2000; in fear versus anxiety? Factors associated with the sition to childhood aggression at age 11 years.
Differential diagnosis includes: Normal variant (if the rest of the ECG looks normal; frequently seen in women due to inaccurate precordial lead placement (under the breast – interspace lower) LVH (look for voltage criteria and ST-T changes of LV "strain") Complete or incomplete LBBB (also note the increased QRS duration) Left anterior fascicular block (should see LAD ≥ -45º in frontal plane) Anterior or anteroseptal MI (look for evolving ST-T changes discount cardizem 120 mg online arrhythmia dizziness, and medical history) Emphysema and COPD (look for R/S ratio in V5-6 <1) Diffuse infiltrative or myopathic processes WPW preexcitation (look for delta waves and short PR) Prominent Anterior Forces (PAF) - defined as R/S ratio >1 in V1 or V2 order 60 mg cardizem fast delivery blood pressure garlic. ST Segment Abnormalities General Introduction to ST, T, and U wave abnormalities Basic Concept: the specificity of ST-T and U wave abnormalities is determined more by the clinical circumstances in which the ECG changes are found than by the particular changes themselves. Thus the term, nonspecific ST-T wave abnormalities, is frequently used for ST segment depression and T wave abnormalities when clinical data are not available to correlate with the ECG findings. This does not mean that the ECG changes are unimportant! It is the responsibility of the clinician providing care for the patient to ascertain the importance of the ECG findings. Examples include hereditary long QT syndromes, and Brugada Syndrome. These changes are not abnormalities; they are appropriate in the setting of altered ventricular conduction. ST-T wave changes are called primary if they are independent of the sequence of ventricular depolarization (e. Differential Diagnosis of ST Segment Elevation Normal Variant "Early Repolarization Pattern": Traditionally this “pattern” consisted of concave upwards ST segment elevation ending with symmetrical, large, upright T waves in the lateral precordial leads (see ECG on p78). Recently, however, this “pattern” has been redefined to include end-QRS notching or slurring with or without ST segment elevation (JACC 2015; 66:470). Example: Acute anterior transmural injury – anterior MI (see selected leads below) 79 Note: Persistent ST elevation long after an acute MI suggests failure of reperfusion, a ventricular aneurysm, or an akinetic scar resulting from a healed MI. Coronary spasm can also occur from other precipitants including cocaine overdose. Example: Post-op acute pericarditis; note diffuse, concave-upwards ST elevation, HR 100 bpm, PR segment depression in leads I, V2, V3; PR segment elevation is seen in aVR. Acute Pericarditis The ECG changes of acute pericarditis evolve over time through the following stages (not all stages are seen in every patient): Stage I: concave upwards ST segment elevation in most leads with reciprocal ST segment depression only in aVR. During this stage there may also be atrial injury represented by PR segment depression in many leads and PR segment elevation in aVR (see above example). Hypothermia: note J waves in most leads (note also atrial fibrillation) Other Causes or ST segment elevation: Left ventricular hypertrophy (seen in right precordial leads with large S-waves) Left bundle branch block (seen in right precordial leads with large S-waves) Advanced hyperkalemia (seen in multiple ECG leads with or without wide QRS complexes) II. Differential Diagnosis of ST Segment Depression Subendocardial ischemia (see picture) 81 As illustrated in the simple 2-cell model of cardiac depolarization (from endocardium-to-epicardium) and repolarization (from epicardium-to- endocardium) the relatively flat ST segment represents the plateau phase of the two action potentials when there is no potential difference between them. During subendocardial ischemia the action potentials from ischemic cells are altered in two ways: 1) loss of resting membrane potential (diastolic injury) which affects the TQ segment of the ECG, and 2) altered depolarization and repolarization which results in ST segment depression and T wave inversion (systolic injury) as seen in an ECG lead facing the myocardial wall segment. Modern ECG recording systems interpret TQ segment shifts as baseline artifact and returns the elevated TQ segment back to the original baseline further depressing the ST segment. Normal V5 ECG at rest before exercise (note normal ST-T and U waves) B. J-junctional ST depression due to increased HR (this is not an ischemic change, but represents atrial repolarization extending through the QRS into the ST segment) C. Early subendocardial ischemia (increased J-junctional depression, slowly upsloping ST) D. Horizontal ST segment depression (≥1mm, horizontal, lasting ≥80 ms) E. Downsloping ST depression with T wave inversion; this is usually seen post-exercise when the HR slows. ST segment elevation (this is a manifestation of transmural ischemia) G. U-wave inversion (a very unusual manifestation of ischemia suggesting LAD or L-main disease). When seen, it occurs during recovery when HR slows down. T Wave Abnormalities INTRODUCTION: The T wave is the most labile wave in the ECG. Abnormal T waves including low-amplitude and inverted T waves may be the result of many cardiac and non-cardiac conditions. The normal T wave is usually in the same direction as the QRS except in the right precordial leads (see V1-3 below). T waves in V1 may also be inverted, but are usually upright in V2-6 in adults. Also, the normal T wave is asymmetric with the ascending half moving more slowly than the descending half.
Disruption may occur to the role divisions (jurisdictions) of organisations (e buy cardizem 180mg visa prehypertension values. In the NHS cardizem 60mg overnight delivery blood pressure over 160, actors/change agents are likely to be interfacing with, and having an impact on, both of these. Resistance to change may come from both of these interests. Evidence from our cases suggests that disruption and the imagining of new forms of service was additionally complicated by the fact that in the NHS it is far from a simple matter to map which actors are more embedded in the status quo and which have a greater stake in challenging it. National policies and strategies emanating from senior levels in NHSE profoundly challenge the status quo in terms of the boundaries between primary and acute care. At the same time, front-line clinicians in district general hospitals are often the most passionate advocates of shoring up the status quo in terms of what happens in the acute sector. So, new models of service delivery can come both from apparently entrenched senior actors (such as those instances in cases B, E and F where the top two or three provided the vision and the impetus) and from more marginal actors (as in cases C and D where enthusiastic GPs with no formal place in the CCG hierarchy used their local knowledge to drive a path for change). Neither one could be said to be inherently superior. The latter, ground-up approach, needed to win resources and support from above. Their position in the field means that they can deploy resources based on expertise and local knowledge and can, credibly, bid for contracts from commissioners of a kind which represent new modes of service provision. These new elements may include improved access, extended hours, multidisciplinary teams and an extended range of services in community settings. Our cases revealed instances where clinical leaders within CCGs (e. In these cases, leaders could deploy the allocated resources (managerial and financial) to deliver the plan. However, given the complexity of the NHS, matters were not always quite so simple. Our cases revealed numerous examples of leadership of service redesign where the challenges were more complicated. The CCG might itself support the status quo because unpicking the tangled web of payments, contracts and systems maintenance appeared too daunting and they saw themselves as having more pressing immediate priorities. Commissioning as a platform for clinical leadership The second question asked about the extent and nature of the scope for clinical leadership and engagement in service redesign that is possible and facilitated by commissioning bodies. This question places the focus on the enabling conditions. Nor did clinicians engage in any meaningful way with these bodies. Representatives from CCGs at HWBs tended to be accountable officers and/or chairpersons. Of more direct interest was the role of the CCGs themselves. The first of these was within the CCGs: how much influence were clinicians able to exercise? The second aspect was the power and influence of CCGs as institutions: what weight did they carry among the many other players in the landscape? There were a significant number of cases where managers acted as the most influential players. However, this was by no means a universal phenomenon. Our data point to cases where GPs exercised extensive influence over the strategic direction of the CCG as a whole and significant influence within specific service areas. In some of the cases this was because influential clinical figures took up roles as chairpersons or accountable officers and steered the CCG in a particular strategic direction. The case studies which focused on reform of primary care, for example, illustrated how leading clinician managers occupying hybrid roles pursued the kinds of changes which reflected the visions set out in Liberating the NHS3 and those wanted by NHSE. The puzzle is why there were not more cases of this kind. The answer stems not only from the expected difficulties in carrying along the GP membership but, additionally, from the complex interplay of diverse institutions each with their power basis and each part of a wider web of services underpinned by payment mechanisms, which were found to be difficult to unravel. The scope for service redesign using the mechanism of these local commissioning groups was thus checked by numerous sources of inertia.
9 of 10 - Review by I. Folleck
Votes: 303 votes
Total customer reviews: 303

Detta är tveklöst en av årets bästa svenska deckare; välskriven, med bra intrig och ett rejält bett i samhällsskildringen.
Lennart Lund